Learning objectives
- What are Aortic Arch Plaques
- Recognition of Aortic Arch Plaques
- Treatment of Aortic Arch Plaques
|
Introduction
- Risk factor and mechanism for stroke and peripheral embolism
- Due to aortic arch atheroma
- Potential cause of cryptogenic embolic stroke
Aetiology
- Approximately 45% of individuals aged ≥ 45 years harbor atherosclerotic plaque in their aorta
- Large, ulcerated, noncalcified, or mobile atheromas, occur in 8% of the population,
- These have been particularly linked with stroke.
- Potential cause of cryptogenic embolic stroke
| Stroke rates in trials were very low at only 2% per annum |
Clinical
- Systemic embolic including stroke
- Sudden onset affecting anterior and posterior circulation
- May cause systemic embolisation
Risk Factors from Plaque Morphology
- Atheroma Greater than 4 mm in thickness
- Ulceration of plaques
- Mobile components
- High degree of protrusion into lumen
|
investigations
- FBC, U&E, ESR and CRP may be elevated.
- Transoesophageal echocardiography can identify plaque
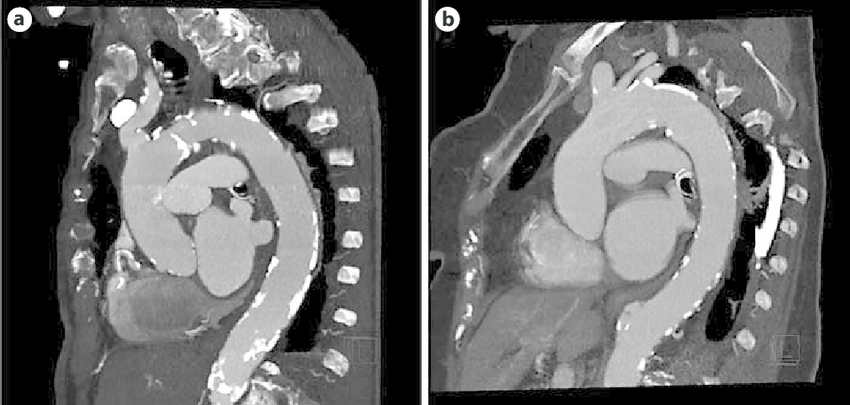
- CT Angiography of the Aorta Is Superior to Transoesophageal Echocardiography
Examples of aortic plaque detection by ECG-triggered CTA in sagittal oblique maximum-intensity projection of the aorta
Differential
Management
- There have been several trials trying to look at this. The ARCH trial randomised patients with TIA or minor stroke who had significant aortic plaques to either warfarin or the combination of aspirin and clopidogrel. This trial was stopped because it turned out that the trial would never reach the power for a definite result. The outcome was that there was a small benefit in favour of aspirin plus clopidogrel vs warfarin, which was not statistically significant. Unfortunately, we still don't know what the best treatment is for patients who have aortic plaques with TIA or minor stroke. A more recent [link] trial looked at aspirin 75 to 150 mg/d plus clopidogrel 75 mg/d over warfarin therapy and found no conclusive evidence as the study despite enrolling over 300 patients was underpowered. The current balance would then be towards DAPT unless there are indications for warfarin.
- Manage atherosclerotic risk factors - statins, diet, smoking, BP reduction, lipids, exercise
- Currently, there is uncertainty as to what this should be, but either combination antiplatelet therapy (aspirin plus clopidogrel) or anticoagulation with warfarin (target INR 2.0-3.0) are commonly used. Statin to lower cholesterol and good BP control.
References
|
|
Note: The plan is to keep the website free through donations and advertisers that do not present any conflicts of interest. I am keen to advertise courses and conferences. If you have found the site useful or have any constructive comments please write to me at drokane (at) gmail.com. I keep a list of patrons to whom I am indebted who have contributed. If you would like to advertise a course or conference then please contact me directly for costs and to discuss a sponsored link from this site.
|