Learning objectives
|
Introduction
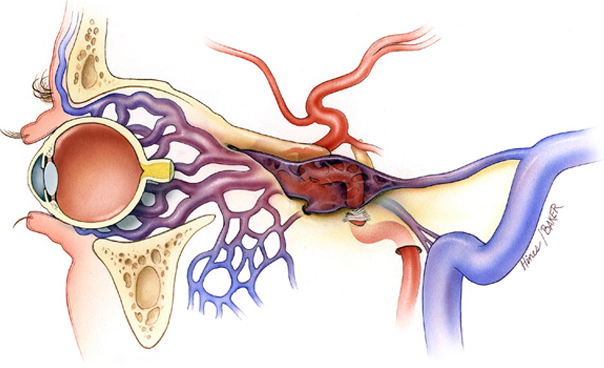
- Anomalus connection between carotid artery and cavernous sinus
- Carotid artery passes through the cavernous sinus
Aetiology
- Form of a dural AV fistula or Rupture of Carotid Aneurysm or AVM in cavernous sinus
- Direct fistulas occur from a tear in the cavernous segment of the ICA or, less commonly, from the intracavernous rupture of an ICA aneurysm.
- Risk - Ehlers Danlos, Pseudoxanthoma elasticum
- May follow a head injury
| Acute onset of pulsatile tinnitus - listen for it may be seen in high flow fistulas which may need urgent intervention so pleae listen of suspected |
Clinical
- May have sudden onset of pulsatile tinnitus and present to ENT with the pulse
- Audible bruit can be heard over skull if shunt large
- Altered acuity as venous back pressure on ophthalmic veins
- Severe cases pulsatile exophthalmos, papilloedema, chemosis, glaucoma
- Damage to III/IV/VI which are also in the lateral wall of cavernous sinus
- Varix of the cavernous sinus and pseudoaneurysm can both present with subarachnoid haemorrhage.
Investigations
- CT head: May be normal or can show some orbital oedema and exophthalmos
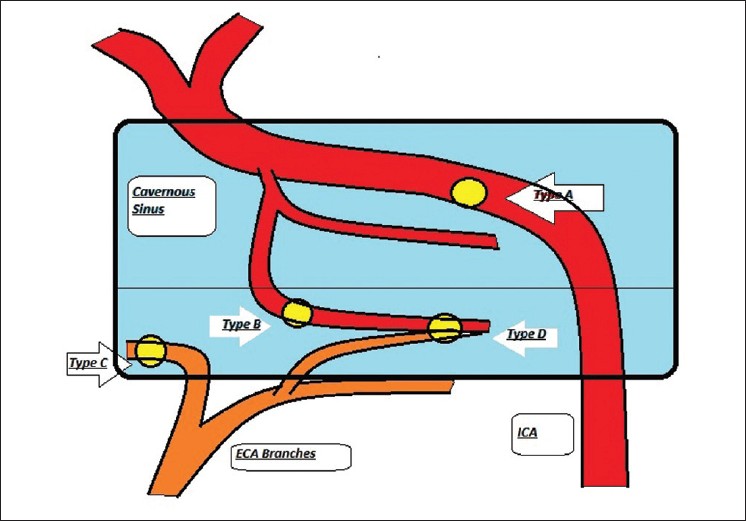
- CTA is optimal for Type A. MRA is superior in Type B, C and D and in demonstrating venous channels which are very important in predicting prognosis and optimal method of management
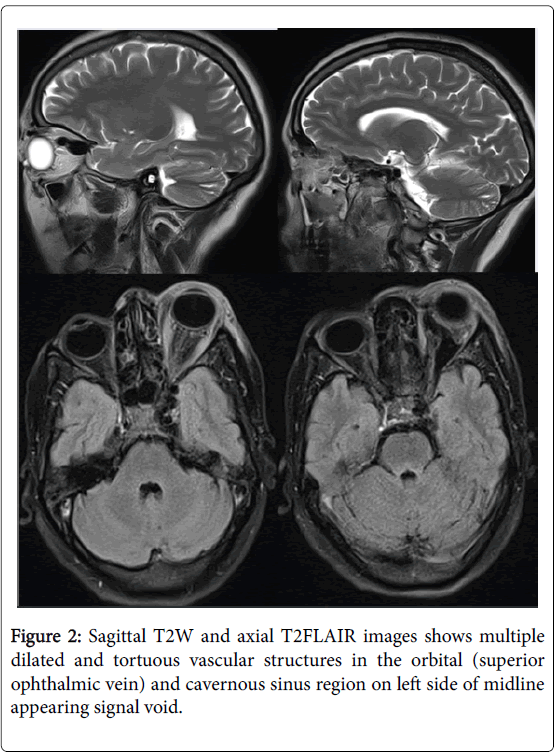
- Noncontrast MRI may reveal enlarged cavernous sinus with multiple flow voids and dilated ophthalmic veins with soft tissue stranding in intraconal and extraconal orbital fat without obvious signs of any obvious mass lesion.
- Contrast-enhanced images with MRA/V: may reveal enlarged cavernous sinus; dilated superior and inferior ophthalmic veins with their draining tributaries and multiple, tiny, dilated arteries within the early enhancing cavernous sinus. Angiographic differentiation between a cavernous sinus varix and a pseudoaneurysm
- Cerebral angiography is still considered as a gold standard for diagnosis of CCF especially in pretreatment planning which shows filling of venous sinuses during the arterial phase, retrograde flow from cavernous sinus to ophthalmic veins and enlarged draining veins
Differential
- Eye signs and Graves disease but eye disease in hyperthyroidism typically occurs bilaterally
 |
 |
| Classification |
|---|
|
 |
Management
- ABC and ITU care if any SAH or significant bleed from rupture. Consider Neurosurgical referral and consideration for endovascular therapy.
- Transarterial embolisation with wide variety of embolising material is management of choice for high-flow, direct CCF
- Those with low-flow, indirect CCF may either undergo spontaneous closure or may require transarterial as well as transvenous approach. They may be given reassurance, educated regarding potential changes in symptoms, and allowed time for potential spontaneous closure of the fistula
References and further reading
- Gemmete JJ, Chaudhary N, Pandey A,Ansari S (2010) Treatment of carotid cavernous fistulas.Current Treatment Options in Neurology12:43-53.
- Korkmazer B, Kocak B, Tureci E, Islak C, Kocer N, et al. (2013) Endovascular treatment of carotid cavernous sinus fistula: A systematic review.World J Radiol 5: 143-155.
| Note: The plan is to keep the website free through donations and advertisers that do not present any conflicts of interest. I am keen to advertise courses and conferences. If you have found the site useful or have any constructive comments please write to me at drokane (at) gmail.com. I keep a list of patrons to whom I am indebted who have contributed. If you would like to advertise a course or conference then please contact me directly for costs and to discuss a sponsored link from this site. |