Learning objectives
- What is Susac syndrome
- Recognition of Susac syndrome
- Treatment of Susac syndrome
|
Introduction
- This syndrome was first described by John O. Susac in 1979
- Unusual an acute autoimmune neurological syndrome
- A rare microangiopathy of brain, retina, cochlea affecting mainly young women
The classical Triad
- Subacute encephalopathy
- Retinal arteriolar branch occlusions
- Sensorineural hearing loss
|
Aetiology
- Small microangiopathy with microinfarctions of cochlear, retinal and encephalic tissue
- Favours the corpus callosum
- Anti-endothelial cell antibodies
Clinical
- Headache, Memory loss, personality change, delirium, confusion
- Ataxia, Acute hearing loss, Encephalopathy, seizures, migrainous headache
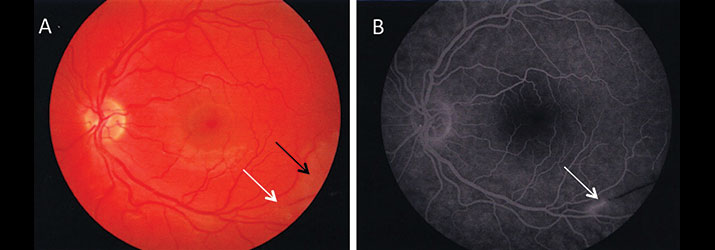
- Acute visual loss - branch retinal artery occlusions
- Clinical course is usually self-limited, fluctuating, and monophasic which may worsen during pregnancy
- Lasts 2-4 years but can be longer or shorter
- Bilateral sensorineural hearing loss which is asymmetric and is thought to reflect sequelae of microinfarction in the apical cochlea
Investigations
- FBC, U&E, CRP may all be normal
- CSF protein can be elevated
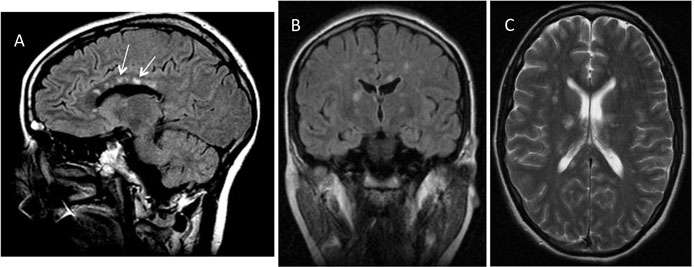
- MRI changes involving central corpus callosum are classic. The lesions are typically small, multifocal, and frequently enhance during the acute stage (70%). Leptomeningeal enhancement was present in 33% and deep grey matter involvement (basal ganglia and thalamus) in 70%. Another article describes changes as Central callosal 'icicle' and 'spoke' lesions in contact with the roof of the callosum and a characteristic string of beads appearance of microinfarcts in the internal capsule have also been recognised. Also called “snowball” lesions in the corpus callosum. Supratentorial Lesions can resemble a "string of pearls".
- Fluorescein angiography: as BRAOs may be diagnostic
- Audiogram: may detect sensorineural hearing loss and should be done even if bedside hearing tests are normal. It may show bilateral low frequency hearing loss, rising to normal at higher frequencies. This is the typical (cochlear) hearing loss seen and reflects microinfarction of the striae vascularis at the apex of the cochlea
 |
 |
Differentials
- Atypical MS/ADEM
- CADASIL/SLE/APL/Vasculitis
- Neuro-Behcet's disease
- Lymphoma, ADEM
- Cerebral vasculitis
- Temporal arteritis or Cogan's syndrome
Management
- Non proven but consider therapies that target both T and B cells - IV Methylprednisolone, Azathioprine, Rituximab, Mycophenolate, IVIG, Plasmapharesis until disease settles.
- Intratympanic injection of dexamethasone in the acute phase of hearing loss and tinnitus may provide transient benefit
- Serial audiometry, flourescin angiography, and MRI to assess response and progression.
- Most make a recovery
References and further reading
|
|
Note: The plan is to keep the website free through donations and advertisers that do not present any conflicts of interest. I am keen to advertise courses and conferences. If you have found the site useful or have any constructive comments please write to me at drokane (at) gmail.com. I keep a list of patrons to whom I am indebted who have contributed. If you would like to advertise a course or conference then please contact me directly for costs and to discuss a sponsored link from this site.
|