Learning objectives
|
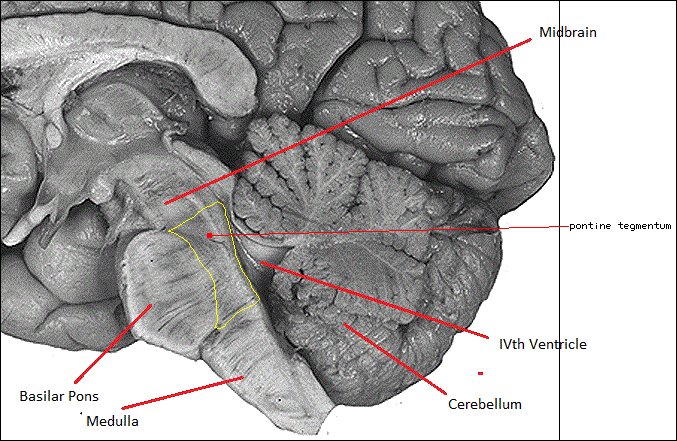
Ventrally rather bulbous due to large cell groups and fibres running transversely between large pontine nuclei and the cerebellum. Laterally lies the bulging middle cerebellar peduncle. The pontine nuclei mediate fibres coming from cerebral cortex to the cerebellum. The VI, VII, VIII and V nerves all leave ventrally. As its name suggests it is bridge like and like any bridge it is a major crossover centre for fibres carrying signals bidirectionally from above and below and communication with the cerebellum. Like any bridge it covers the CSF filled 4th ventricle which separates it from the cerebellum with its vermis and hemispheres which sit tightly behind.
The Pons contains the Corticospinal fibres, Corticopontine fibres, Pontocerebellar fibres and Raphe nuclei. The lower Pons contains the Nucleus of VI, Nuclei of VII, Facial nerve, Superior salivatory Gustatory. The facial nerve and abducent nerve are closely associated as the exiting VII nerve loops around the nucleus of VI. Also contained is the Medial lemniscus (carries contralateral dorsal column), Spinothalamic tract (carries pain and temperature) and Middle cerebellar peduncle which contains fibres from c/L pons to cerebellum.
Medial structures
- Medial longitudinal fasciculus
- VI (Abducent) nerve nucleus and fibres
- Genu of VII (Facial) closely associated with VI
- Medial lemniscus (carries contralateral dorsal column)
- Corticospinal tract
Lateral structures
- Facial nucleus VII and nerve fibres
- Spinal nucleus and tracts of V
- Lateral spinothalamic tract (spinal lemniscus)
Aetiology
Pontine strokes are usually due to occlusion of leg from small perforating arteries or to obstruction at the basilar level of the ostia or even total basilar artery occlusion. It is seen in those with hypertension and diabetes and in an older age group. Occasionaly there may be an underlying vascular anomaly. Ischaemic strokes appear to respect the midline. The fact that the fourth ventricle lies behind the pns means that any swelling here or bleeding into the ventricle can result in obstructive hydrocephalus which may require shunting. Strokes can damage the corticospinal, corticopontocerebellar, and corticobulbar tracts as well as other structures.
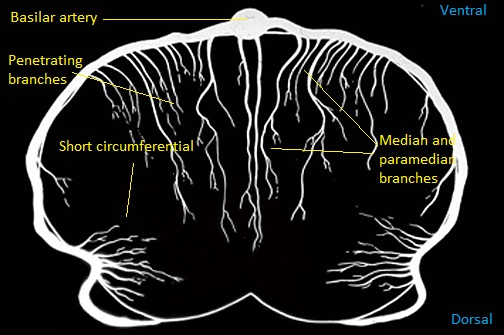
Vascular supply
- From the basilar artery which lies anteriorly and provides median and paramedian perforators.
- Short circumferential branches irrigate more laterally
- Middle cerebral peduncle is supplied by branches of the superior cerebellar and anterior inferior cerebellar arteries.
Pontine Symptoms
- Comatose, locked in syndrome with preservation of upward gaze, Pinpoint pupils
- Pyrexias and autonomic dysfunction
- LMN or UMN VIIth which is ipsilateral.
- Diplopia, Lateral gaze palsy if VIth nerve affected
- Variants of Quadriparesis due to corticospinal involvement
- There may be waxing and waning of symptoms initially like a capsular warning syndrome
- Sensory symptoms
- Dysarthria - Clumsy hand type Lacunar syndromes
- Vertigo, Dizziness due to involvement of cerebellar peduncles
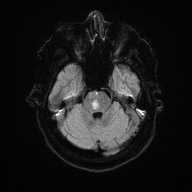
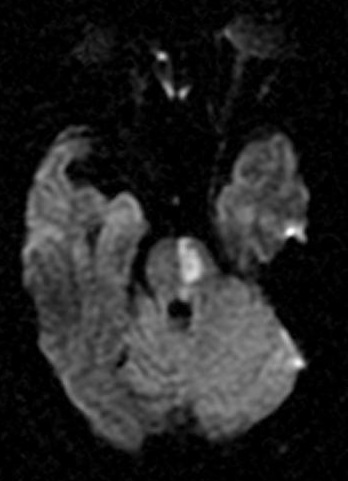
Pontine Infarction
Pontine strokes are usually unilateral and reflect small vessel occlusion of penetrating vessels. Occasionally a basilar artery occlusion blocking the ostia can result in bilateral infarction as can be seen below. Small vessel strokes share same risk factors as small vessel disease elsewhere with hypertension, diabetes and age as significant risk factors. Large vessel basilar infarcts also share the same risk as other large vessel strokes including localised atherosclerosis and embolism. The fact that the fourth ventricle lies behind the pons means that any swelling here can result in obstructive hydrocephalus which may require shunting.
 |  |
 |  |
Pontine Haemorrhage
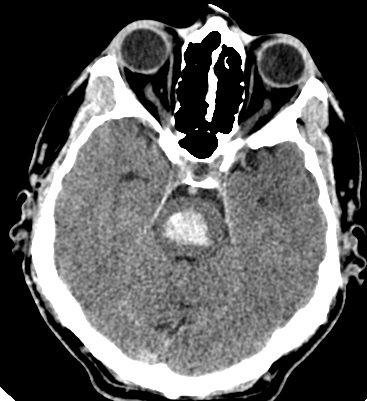 | 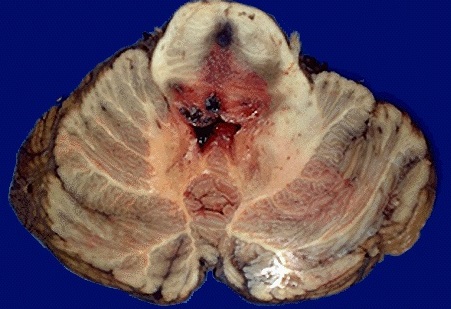 |
Bleeding into the pons is associated with a high fatality up to 50%. Try to establish the cause which is often hypertension but may also be due to a AVM or Cavernoma which may do better. Clinically most patients will be comatose depending on the extent of brainstem damage and there may be Pontine and other brainstem signs with diplopia, nystagmus, nausea, vomiting. The main investigation is non-contrast CT initially which should be sensitive enough to pick up posterior fossa blood and then follow up with MRI/MRA. Management is traditionally conservative. Outcome is hard to predict, some patients do very well and others less so. In a younger patient it may be reasonable to intubate and ventilate and see what happens. The fact that the fourth ventricle lies behind the pons means that any swelling here or bleeding into the ventricle can result in obstructive hydrocephalus which may require shunting.
| Note: The plan is to keep the website free through donations and advertisers that do not present any conflicts of interest. I am keen to advertise courses and conferences. If you have found the site useful or have any constructive comments please write to me at drokane (at) gmail.com. I keep a list of patrons to whom I am indebted who have contributed. If you would like to advertise a course or conference then please contact me directly for costs and to discuss a sponsored link from this site. |