Themes: Hyperacute Care, Thrombolysis, Complications.

| Bill is a 72 year old male who was admitted with Left hemiparesis and Left hemisensory loss and an NIHSS of 13. It is a presumed Right MCA infarct. He is in a hospitals which does not offer thrombectomy. He normally takes Aspirin 75 mg for IHD and Enalapril for hypertension. The CT shows a small clot in the right MCA. His BP is 190/120 mmHg. The plan is to give him Alteplase. What would you do next. |
|---|

1. What treatment would you offer for the high blood pressure
First of all check that there is no other cause for his high BP such as anxiety and a full bladder or pain. Consider a small dose of Labetalol 10-20 mg slow IV to lower his BP. BP must be less than 185/110 mmHg to give Alteplase. If this fails to lower the BP then consider increasing the dose or giving an infusion.
2. What advice would you say to HASU staff
Yes it would now be safe to start Alteplase but to check the BP every 15 mins and if the BP exceeds 185/110 mmHg in the next 12 hours to consider further IV Labetalol. In some cases I have given oral BP meds e.g. Amlodipine 5 mg to keep BP controlled during thrombolysis when I was concerned. I would also get an anaesthetic review to just watch his airway. BP often settles when patients get onto a quiet ward or if there is pain that needs treatment or urinary retention needing a catheter.
You give a total of Labetalol 20 mg and now his BP is 160/100 mmHg and he is given Alteplase
|
|---|
3. You look in his mouth.

There is marked unilateral swelling of the tongue.
4. What would you do now.
- ABC, Stop the Alteplase. Alert anaesthetic team if airway concerns.
- If there was wheezing, stridor, rash/urticaria, cyanosis, or hypotension then treat as acute anaphylaxis
- he would be given IM Adrenaline and IV Hydrocortisone and IV fluids.
- In most cases it does not compromise respiratory function and can be conservatively managed.
- The oedema is usually mild, transient and contra-lateral to the site of ischaemia
- Oedema more significant if bilateral and can make intubation difficult.
- Often there is CT evidence of ischaemia in the insular and frontal cortex
- Angioneurotic oedema is seen more commonly in those on an ACEI due to elevated Bradykinin levels.
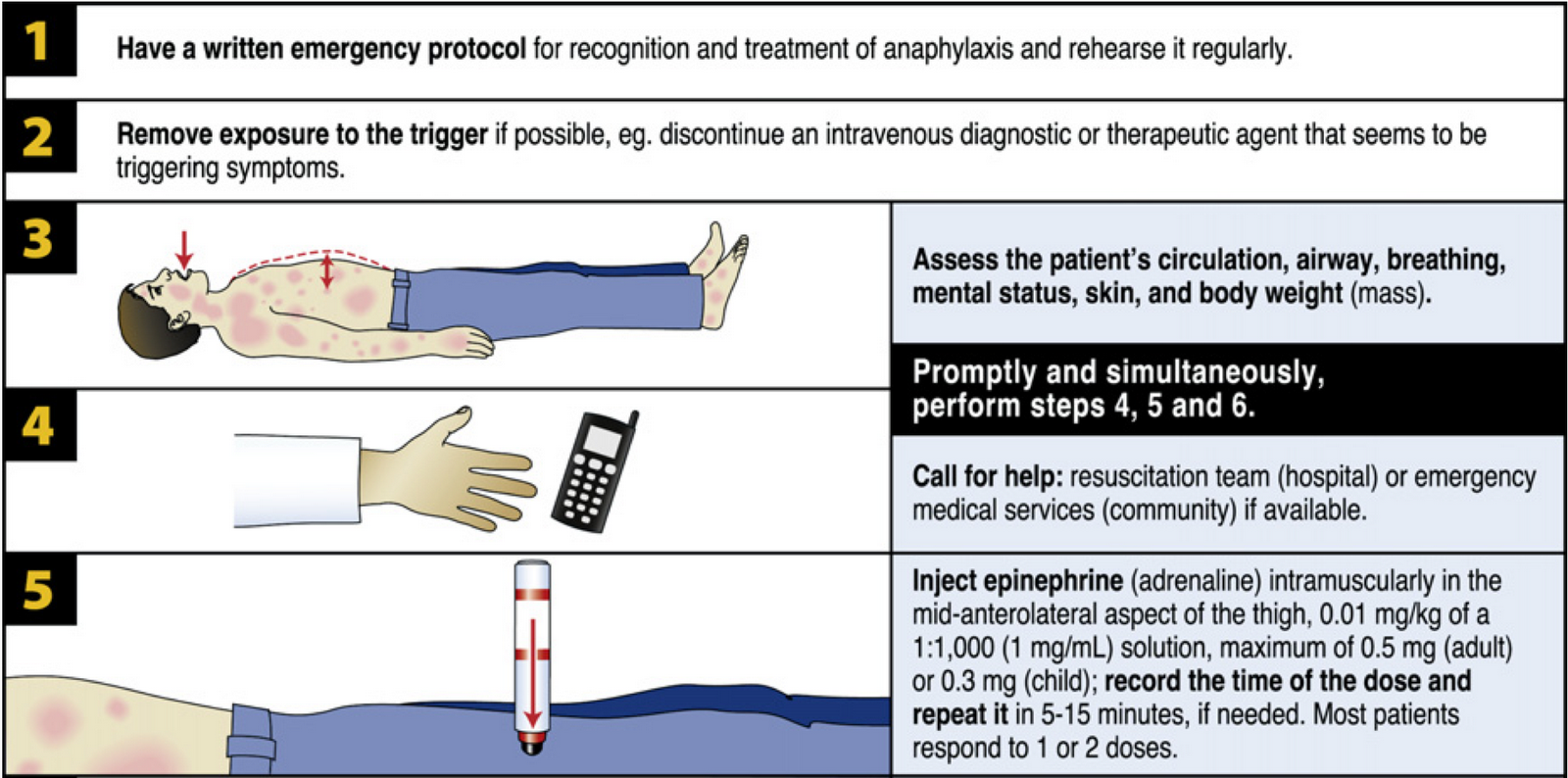
5. How is Adrenaline given.
It is given as Adrenaline 0.5 mg of 1 in 1000 IM into the Anterolateral thigh. The volume is usually 0.5 ml. It may be repeated if there is no initial response after 5 mins. Press over the site if there has been significant alteplase given to minimise haematoma formation.
6. He is moved to ITU for observation overnight. The ITU team ask when he can have aspirin and as he is NBM what fluids to give him
- You calculate that he only had 10% of his Alteplase which was stopped in view of the reaction.
- In view that bleeding would be unlikely so you decide that he can have it now.
- He receives Aspirin 300 mg PR as he is Nil by mouth (NBM).
- He is commenced on 1 Litre of N-Saline over 8 hours.
- Due to the tongue swelling his swallowing assessment is deferred to the next day
- He settles and has an uneventful night and is moved to the HASU the next morning
Next: >> Clinical Scenario 5: next
| Note: The plan is to keep the website free through donations and advertisers that do not present any conflicts of interest. I am keen to advertise courses and conferences. If you have found the site useful or have any constructive comments please write to me at drokane (at) gmail.com. I keep a list of patrons to whom I am indebted who have contributed. If you would like to advertise a course or conference then please contact me directly for costs and to discuss a sponsored link from this site. |